

Return to Work Programs
Quick Answer
A return-to-work program is a written process that brings injured employees back to safe, productive duty as their medical restrictions allow — often through modified work. Coordinating employer, worker, physician, and adjuster, it shortens claim duration, converts lost-time claims into medical-only ones, protects your experience modification factor, and retains experienced staff.

How to Build a Return-to-Work Program
A return-to-work Program is a structured, written process that brings an injured employee back to productive work as safely and as quickly as their medical restrictions allow — typically through temporary transitional, light, or modified duty. A well-run return-to-work program coordinates four parties who rarely talk to one another on their own: the employer, the injured worker, the treating physician, and the workers' compensation claims adjuster. Its purpose is to move recovery out of the living room and back into the workplace, where it is faster, cheaper, and far more likely to end with the employee still on your payroll.
Core Components of a Return to Work Program
- A Written Policy: A documented return-to-work policy that states the company's commitment to transitional duty, defines who is eligible, sets the maximum duration of an assignment, and is distributed to every employee — not kept in a binder in the HR office.
- Essential-Function Job Descriptions: Physical demand descriptions for each position — lifting limits, standing time, reaching, climbing, keyboarding — that the treating physician can actually read and respond to. Without them, doctors default to "off work."
- A Transitional Duty Job Bank: A pre-built inventory of real, productive tasks that can be assembled into temporary assignments matching common restriction patterns, so nobody is inventing a job under pressure the day the release arrives.
- A Written Job Offer: A formal, dated letter describing the transitional assignment, its hours, its pay, its restrictions, and its expected duration — delivered to the employee and copied to the adjuster and the physician.
- Communication Protocol: A defined cadence of contact with the injured employee from day one, so the worker stays connected to the workplace instead of drifting into disability.
Overview of Related Topics
- Transitional, Light, and Modified Duty: Three terms used interchangeably in conversation that mean meaningfully different things in a claim file — and the distinction drives how you document the assignment.
- The Interactive Process: The ADA's required back-and-forth dialogue with an employee whose injury rises to the level of a disability — triggered far more often by workers' compensation claims than most employers realize.
- Workers' Comp, ADA, and FMLA Overlap: A single work injury can trigger all three laws simultaneously, each with its own obligations, and compliance with one does not satisfy the others.
- Cost and Experience Modification: Lost-time claims drive indemnity payments and the experience modification factor, which in turn drives your workers' compensation premium for the next three years.
- Measurement: Return-to-work rate, average lost days per claim, claim duration, and modified-duty utilization are the metrics that tell you whether the program is actually working.
Return to Work Defined
Return to work (RTW) is the coordinated process of returning an employee who has been absent due to a work-related injury or illness to productive employment — either to their pre-injury job, to that job with modifications, or to a temporary transitional assignment — under the supervision of the treating physician's documented restrictions. It is both a medical outcome and an administrative discipline. The medical side is owned by the doctor. The administrative side is owned by the employer, and that is where most programs succeed or fail.
Return to Work vs. Stay at Work
The two terms describe different moments in the same claim and are frequently confused. Stay at work means the employee never leaves. The injury occurs, restrictions are issued, and the employer immediately adjusts duties so that the worker remains on the job without a single lost day. Return to work means the employee has already been out — the claim has become a lost-time claim — and the process now involves bringing them back after an absence.
The distinction matters financially. A stay-at-work outcome typically keeps the claim as a medical-only claim, which is dramatically less expensive and, under most experience rating formulas, carries far less weight against your experience modification factor. Once an employee crosses the threshold into lost time and begins collecting indemnity benefits, the claim's cost and its rating impact both rise sharply. The best return-to-work programs are therefore aggressive about the first 24 to 72 hours, because the cheapest lost-time claim is the one that never becomes a lost-time claim at all.
Key Terms Employers Should Know
- Work Status Report: The physician's written statement of what the employee can and cannot do — the single most important document in the entire process.
- Restrictions: Specific physical or cognitive limits (e.g., "no lifting over 15 pounds," "no overhead reaching," "sit/stand at will") that define what work is permissible.
- Maximum Medical Improvement (MMI): The point at which the employee's condition has stabilized and is not expected to improve further. Restrictions in place at MMI may be permanent.
- Temporary Total Disability (TTD): Wage-replacement benefits paid while the employee is completely unable to work. Every day of TTD is a day the return-to-work program is losing money.
- Temporary Partial Disability (TPD): Benefits paid when the employee returns to work at reduced hours or reduced wages — often the direct financial result of a transitional duty assignment, and far cheaper than TTD.
- Functional Capacity Evaluation (FCE): A structured assessment of what the employee can physically do, used to resolve disputes about restrictions or to establish permanent limitations.

Transitional, Light, and Modified Duty: What's the Difference?
These three terms are used interchangeably in break rooms and on claim files, and not being precise creates real problems. When an employer tells an adjuster "we put him on light duty" but means "we gave him his own job with a lifting restriction," the claim gets coded incorrectly, the benefit calculation may be wrong, and the documentation trail becomes indefensible if the assignment is later challenged. Precision here is not being picky — it is claims management.
The Three Definitions
- Modified Duty: The employee returns to their own job, with specific tasks altered, removed, or reassigned to accommodate restrictions. The job title, the department, and usually the pay stay the same. A machine operator who continues running her machine but has a coworker handle the 50-pound material loads is on modified duty.
- Light Duty: The employee is placed in less physically or mentally demanding work than their normal job. It may be a different set of tasks entirely. The EEOC uses this term broadly to describe work that is physically or mentally less demanding than the employee's regular duties, and it may be temporary or permanent depending on how the employer structures it.
- Transitional Duty: A time-limited assignment with a defined endpoint and an explicit goal of progressing the employee back to full duty. The word "transitional" carries the most important idea in the entire discipline: this is a bridge, not a destination. It has a start date, a review date, and an expiration date.
Most well-designed programs standardize on transitional duty as the operating term, precisely because it builds the time limit into the process. An assignment that is described as "light duty" with no end date has a way of becoming a permanent second job classification — one that the employer never intended to create and may later have difficulty removing.
Building a Transitional Duty Job Bank
The single most common reason a return-to-work program fails is that no one can think of anything for the injured employee to do. The solution is to think of it in advance, when there is no injured employee waiting and no pressure in the room. A transitional duty job bank is a written inventory of real, productive tasks — already needed by the business, already on someone's someday list — that can be assembled into temporary assignments.
- Inventory the Work Nobody Gets To: Inventory counts and cycle counts, tool crib organization, safety audits and housekeeping inspections, equipment inspection logs, parts kitting, filing and document scanning, customer follow-up calls, inventory of PPE stock.
- Map Tasks to Restriction Patterns: Group tasks by what they require. A sedentary bank (phone, data entry, review work). A no-lifting bank. A no-overhead-reaching bank. A limited-standing bank. When a work status report arrives, you match rather than brainstorm.
- Involve Supervisors in Building It: The supervisors who will host these assignments should help construct the bank. A task list produced by HR in isolation gets rejected on the floor as busywork.
- Document Physical Demands for Each Task: Each bank entry should state its own physical demands, so the assignment can be matched to restrictions objectively and defended later if the employee, the physician, or the adjuster questions it.
- Keep It Productive: If the task would not otherwise be worth paying someone to do, it does not belong in the bank. Make-work destroys the credibility of the entire program — for the injured employee and for everyone watching.

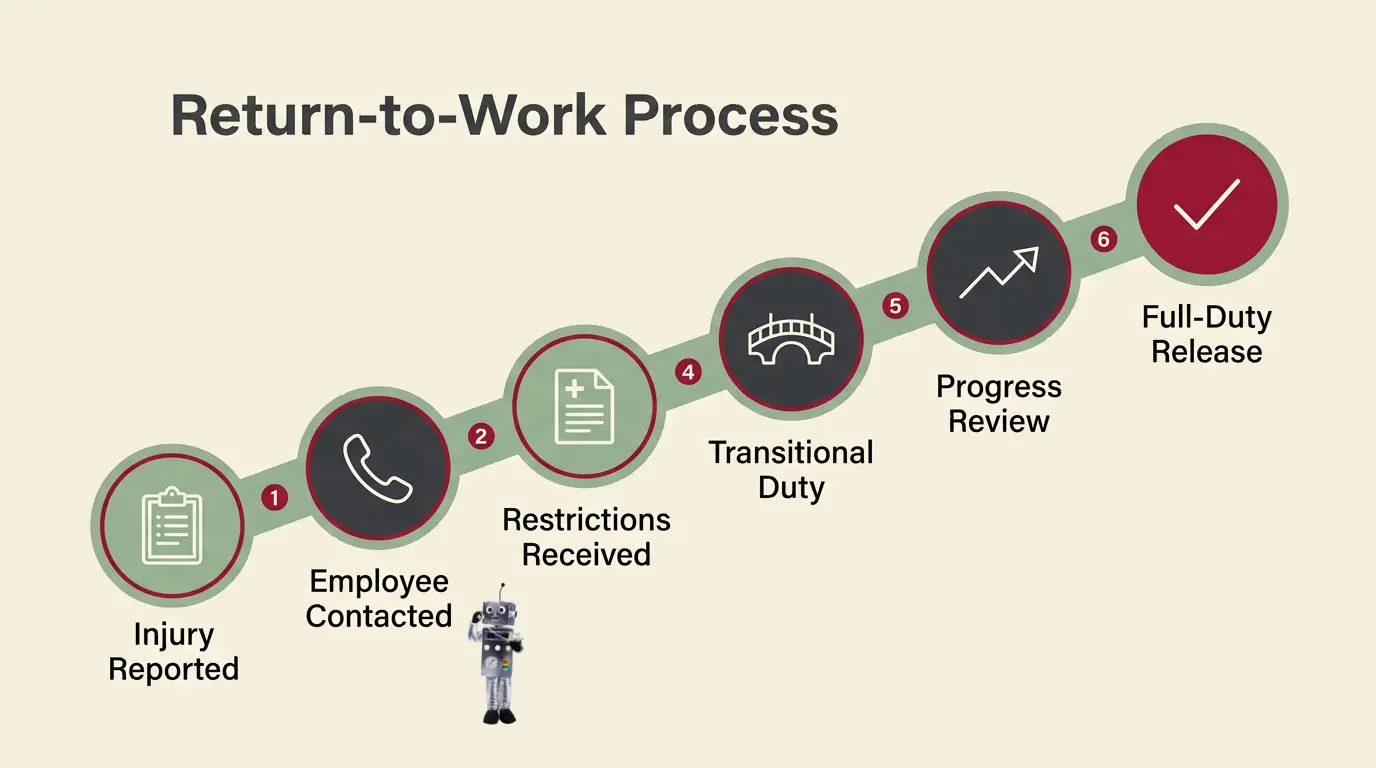
Step-by-Step Guide: Running a Return-to-Work Claim
A return-to-work program is a sequence, and the sequence is the same on every claim. What varies is how quickly and how consistently the employer executes it. The steps below describe the process from the moment an injury is reported to the moment the employee is released to full duty.
- Report the Injury Immediately. Reporting lag is the single strongest predictor of a claim that goes long. Report to the carrier or PEO within 24 hours. Delayed reporting drives up medical cost, invites attorney involvement, and destroys the employer's ability to influence the early medical direction of the claim.
- Make Contact With the Employee Within 24 Hours. Not a claims call — a human one. The supervisor or HR calls to ask how the employee is doing and to say, clearly, that there will be a place for them and that the company intends to bring them back. Employees who feel abandoned in week one are the employees who hire attorneys in week three.
- Send the Job Description to the Treating Physician. Physicians write "off work" when they do not know what the job requires. Send the essential-function job description with physical demands and a copy of your transitional duty policy stating that the company can accommodate restrictions. This one step changes more outcomes than any other.
- Obtain the Work Status Report. After every appointment. The employee should be required by policy to deliver it — or the clinic should be authorized to send it directly — the same day. No work status report, no assignment.
- Match the Restrictions to a Transitional Assignment. Go to the job bank. Identify a task set that fits inside the restrictions with room to spare. Do not push the boundary of the restrictions; a re-injury on transitional duty is a catastrophe for the claim and for the program's credibility.
- Put the Offer in Writing. A dated letter stating the assignment, the specific tasks, the hours, the shift, the pay rate, the restrictions being accommodated, the reporting location and supervisor, and the expected duration. Give a copy to the employee, the adjuster, and the physician's file. A verbal offer is, for practical purposes, no offer at all.
- Brief the Supervisor Before Day One. The receiving supervisor needs to know exactly what the employee may and may not do, that the restrictions are not negotiable, and that undermining the assignment — through comments, through pressure, or through quiet exclusion — is a serious performance issue.
- Monitor the Assignment. Check in during the first shift, and weekly thereafter. Document what the employee actually did. If the employee reports increased pain, escalate to the physician immediately rather than pushing through.
- Review and Progress the Assignment. Transitional duty is a ramp, not a plateau. As restrictions loosen at each medical appointment, the assignment should expand toward the pre-injury job. Set a review date — commonly every two weeks — and hold it.
- Return to Full Duty — and Close the Loop. Obtain a written full-duty release before returning the employee to unrestricted work. Then debrief: what caused this injury, and what in the workplace still causes it? A return-to-work program that never feeds information back into safety is treating symptoms.

Roles & Responsibilities
Return-to-work programs do not usually fail because someone did their job badly. They fail at the handoffs — between the clinic and the employer, between HR and the supervisor, between the adjuster and the injured worker. Naming the owner of each role, in writing, is what closes those gaps.
The Injured Employee
- Reports the injury promptly and attends all scheduled medical appointments.
- Delivers the work status report to the employer after every appointment.
- Reports to the transitional assignment and works within — and only within — the documented restrictions.
- Communicates changes in condition to both the employer and the treating physician rather than working through pain.
The Direct Supervisor
- Makes first contact after the injury and maintains the relationship during the absence.
- Hosts the transitional assignment and enforces the restrictions on the floor — including protecting the employee from well-meaning coworkers who ask for "just one" lift.
- Documents what the employee actually performed each day.
- Escalates immediately if the assignment is not working or if restrictions appear to be exceeded.
Human Resources
- Owns the written policy, the job bank, the essential-function job descriptions, and the offer letters.
- Runs the ADA interactive process when the injury may rise to the level of a disability.
- Tracks FMLA designation and the 12-week entitlement in parallel with the comp claim.
- Maintains the OSHA 300 log and ensures restricted-duty days are recorded correctly.
The Claims Adjuster
- Determines compensability, manages the reserve, and authorizes medical treatment.
- Calculates and pays indemnity benefits — and adjusts them when a transitional offer is made.
- Should receive a copy of every written transitional duty offer, because a valid offer of suitable work can change the benefit picture substantially in most jurisdictions.
The Treating Physician
- Issues the restrictions and the work status report; determines MMI.
- Is entirely dependent on the employer for information about what the job actually requires. A physician working from a job title alone will nearly always be more conservative than one working from a physical demands description.
The Nurse Case Manager and the PEO or Carrier
- A nurse case manager — assigned on more complex claims — coordinates between the medical provider, the employer, and the adjuster, and is often the fastest route to getting a restriction clarified.
- A PEO or carrier provides the claims infrastructure, the reporting, and the return-to-work expertise that most small employers cannot staff internally.

The Interactive Process: A Return-to-Work Roadmap
The interactive process is the ADA's required, good-faith dialogue between an employer and an employee with a disability to identify an effective reasonable accommodation. Employers tend to associate it with non-occupational conditions and are frequently surprised to learn that a workers' compensation injury can trigger it — and that failing to engage in it is itself a source of liability, independent of whether an accommodation was ultimately available.
A work injury does not automatically create ADA obligations. Under EEOC guidance, an employee with an occupational injury has a disability for ADA purposes only if the impairment substantially limits a major life activity, if there is a record of such an impairment, or if the employer regards the employee as having one. But the threshold is lower than most employers assume, and the safest operating posture is to run the interactive process whenever restrictions are significant or extended — not to litigate the definition of disability in your own head.
The Roadmap
- Recognize the Trigger. An extended absence, permanent restrictions, restrictions that keep getting renewed, or an employee request for a change in duties. No special wording is required from the employee — a request for help is enough.
- Meet With the Employee. An actual conversation, documented. Ask what they are having difficulty doing and what they believe would help. The employee is a source of accommodation ideas, not merely a recipient of them.
- Identify the Essential Functions. Work from the written job description. The ADA requires accommodation of essential functions — it does not require you to eliminate them. Marginal functions, however, can be reassigned.
- Obtain the Medical Information You Need — and Only That. You may ask for documentation of the limitation and its expected duration. You may not go fishing through the employee's medical history, and what you do receive must be kept confidential and separate from the personnel file.
- Identify and Evaluate Options. Job restructuring, schedule modification, part-time work, equipment or assistive devices, ergonomic changes, or reassignment to a vacant position for which the employee is qualified.
- Implement, Document, and Follow Up. Choose an effective accommodation — you are not required to choose the employee's preferred one — put it in writing, and revisit it. Accommodations that worked in March may not work in September.
The cost objection is largely mythology. In the Job Accommodation Network's ongoing employer survey, of the employers who provided cost information about accommodations they had implemented, roughly six in ten reported that the accommodation cost nothing at all, and most of the rest involved only a modest one-time expense. (askjan.org)
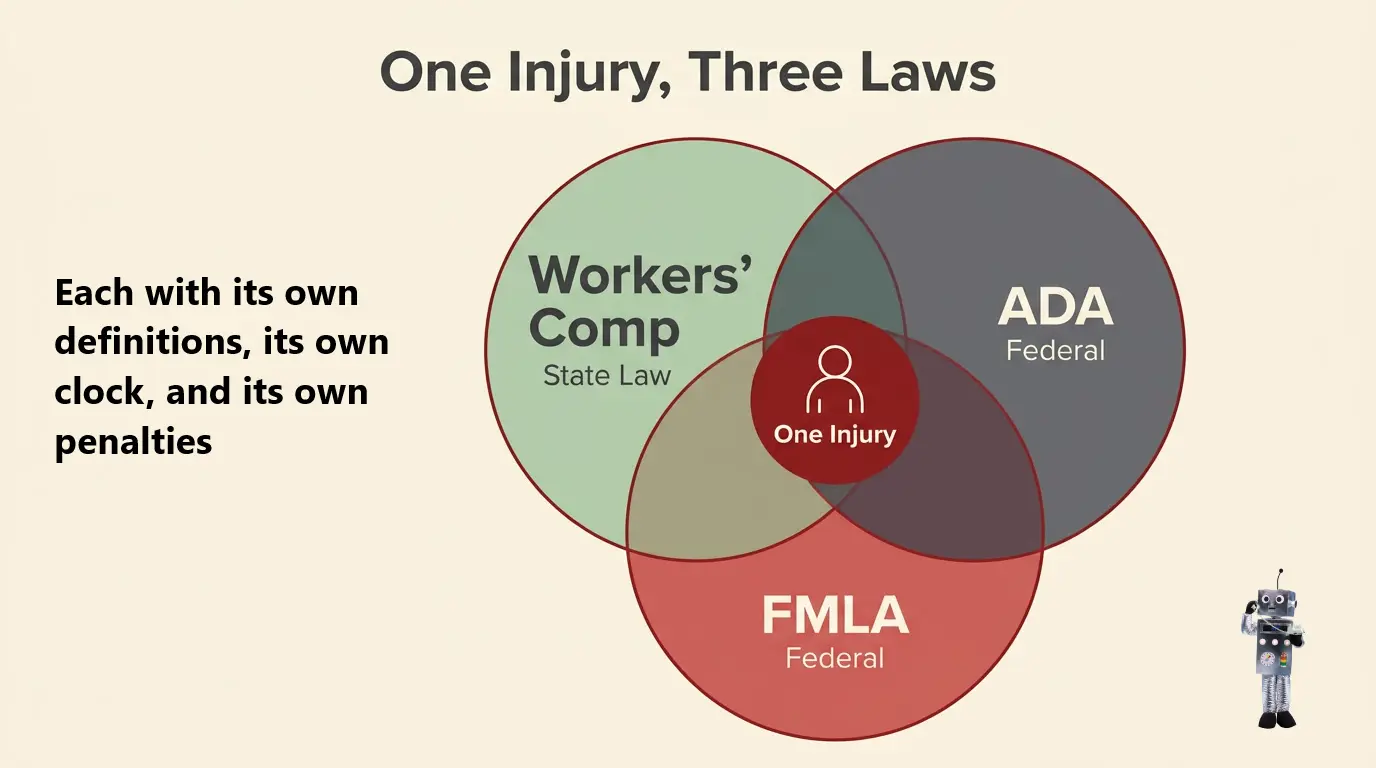

Where Workers' Comp, ADA, and FMLA Intersect
One injury. Three statutes. Each with its own definitions, its own clock, and its own penalties — and compliance with any one of them satisfies exactly none of the others. This is where the majority of return-to-work mistakes are made, and it is worth slowing down.
What Each Law Actually Does
- Workers' Compensation (state law): Pays medical costs and wage replacement for a work-related injury, on a no-fault basis. It says almost nothing about whether you must hold the employee's job open.
- The ADA (federal): Prohibits disability discrimination and requires reasonable accommodation for a qualified employee with a disability — regardless of whether the disability came from a work injury or a weekend fall. Applies to employers with 15 or more employees.
- The FMLA (federal): Provides eligible employees up to 12 weeks of job-protected leave for a serious health condition — which a serious work injury usually is. Applies to employers with 50 or more employees within 75 miles.
The Points Employers Get Wrong
- Workers' comp leave and FMLA leave can run concurrently — but only if you designate it. If you do not send the FMLA designation notice, you may find you have handed the employee 12 weeks of protected leave after their comp leave ends. Designate it, in writing, at the start.
- You cannot force an employee to accept light duty in place of FMLA leave. Light duty work does not count against the FMLA entitlement, and an employee may decline a light duty assignment and remain on FMLA leave. However — and this is the part that surprises people — declining a valid offer of suitable transitional work will typically end or reduce their workers' compensation indemnity benefits under state law. The employee may keep their leave; they may not keep their wage-replacement check.
- You are not required to create a light duty position under the ADA. The ADA does not obligate an employer to create a job that does not exist. But if you reserve vacant light duty positions for occupationally injured workers, EEOC guidance provides that you must consider reassigning an employee with a non-occupational disability into such a vacancy as a reasonable accommodation, absent undue hardship. Reserving light duty exclusively for comp claimants is a common and consequential error. (eeoc.gov)
- "100% healed" policies are a liability. Requiring an employee to be fully recovered with no restrictions before returning is one of the most reliable ways to lose an ADA claim, because it forecloses the accommodation analysis entirely. If the employee can perform the essential functions with a reasonable accommodation, the employer must consider it.
- Being "totally disabled" for comp purposes does not mean unable to work under the ADA. The two systems use the word "disability" to mean different things. A workers' comp disability rating is not an ADA determination, and it does not relieve the employer of the duty to consider accommodation.
- Retaliation is separately actionable. Nearly every state prohibits retaliation against an employee for filing a workers' compensation claim. A termination that follows closely on the heels of a claim will be examined on that timeline, regardless of the reason given.

Return-to-Work Compliance Checklist
Use this as an audit instrument. If you cannot answer yes to an item, that item is where your next claim will get expensive.
Policy & Documentation
- Written return-to-work policy exists, is dated, is included in the employee handbook, and has been acknowledged by employees in writing.
- Essential-function job descriptions with physical demands exist for every position — and are current, not five years stale.
- A transitional duty job bank is documented and maintained, with the physical demands of each task recorded.
- Written transitional duty offer letters are used on every assignment. No verbal offers.
- Transitional assignments carry a stated duration and a scheduled review date. Open-ended assignments are the enemy.
Legal & Regulatory
- FMLA is designated in writing at the outset where the employer and employee are covered and eligible, so that comp leave and FMLA leave run concurrently.
- The ADA interactive process is initiated and documented where restrictions are significant, extended, or permanent.
- No "100% healed" requirement appears anywhere in policy or practice.
- Light duty is not reserved exclusively for occupationally injured employees, or if reserved positions exist, non-occupationally disabled employees are considered for reassignment into them.
- Medical information is kept confidential and stored separately from the personnel file, with access limited to those with a need to know.
- Restricted-duty and job-transfer days are recorded on the OSHA 300 log. This is the item employers most often get wrong: returning an injured worker to restricted duty does not make the case disappear from your log. It remains a recordable DART case, recorded in the job-transfer-or-restriction column, and the days of restriction are counted (capped at 180 calendar days). Return-to-work reduces cost and duration — it does not erase recordability, and treating it as a way to keep cases off the log is a recordkeeping violation.
- State-specific rules are documented for every state in which you have employees — including rules on the validity of a light duty offer, wage-loss benefit offsets, and the maximum duration of transitional assignments.
- No adverse action is taken on the basis of the claim itself. Anti-retaliation protections apply in nearly every jurisdiction.

The Cost of Lost Time: Business Case & Experience Mod Impact
Every employer intuitively understands that injuries are expensive. Fewer understand that the same injury can cost radically different amounts depending entirely on what the employer does in the two weeks after it happens. That difference is the business case for return to work.
What a Claim Actually Costs
Workers' compensation claims carry two cost components. Medical pays for treatment. Indemnity replaces wages while the employee is unable to work. Return-to-work programs have limited influence over the first and enormous influence over the second — and indemnity is where the duration-driven damage compounds. Drawing on NCCI data, the National Safety Council reports that the average cost across all workers' compensation claims for accidents occurring in 2022–2023 was $47,316, with lost-time claims from falls or slips averaging $54,499 and motor-vehicle-related claims averaging $91,433. (injuryfacts.nsc.org)
Those are averages, and averages understate the problem. Claim cost distributions have a long right tail: a small number of claims that stay open for months consume a wildly disproportionate share of the total. Duration is the mechanism. The longer an employee is out, the more likely the claim is to attract attorney involvement, to develop secondary conditions, to end in a permanent disability rating, and to never close cleanly. Time out of work is not a neutral waiting period — it actively degrades the outcome.
The Experience Modification Factor
The experience modification factor — the "e-mod" or "EMR" — is the multiplier applied to your manual workers' compensation premium based on your own claims history relative to businesses of similar size in your industry classification. An e-mod of 1.00 is average. An e-mod of 0.85 means you pay 15% less than a comparable employer; an e-mod of 1.20 means you pay 20% more, on every dollar of premium, for three policy years.
The critical structural feature of experience rating is that it is weighted toward claim frequency and toward the primary (first-dollar) portion of each loss, not toward catastrophic severity alone. In practical terms: a cluster of lost-time claims will move your e-mod more than most employers expect, and each of those claims carries its full primary loss into the calculation. Converting a lost-time claim into a medical-only claim through an immediate stay-at-work assignment does not just save indemnity dollars — in most jurisdictions medical-only claims are discounted in the experience rating formula, meaning the rating impact is reduced as well.
The Compounding Math
- Direct savings: Every day an employee works on transitional duty is a day of indemnity benefits not paid, and a day of productive labor received in exchange for wages you were going to pay in some form anyway.
- Reserve savings: Claims reserves are set based on projected duration. A demonstrated return-to-work program that shortens duration lowers reserves — and reserves, not just paid losses, drive the experience rating calculation.
- Premium savings: A lower e-mod applies to your entire payroll, for three years, on every renewal.
- Retention savings: Replacing an experienced worker who never comes back costs a substantial multiple of what it costs to bring them back on restricted duty for six weeks.
- Litigation avoidance: The employee who is contacted on day one, offered work in week two, and treated as a valued member of the team is not the employee who calls a plaintiff's attorney.

Return to Work in a Small Business
The objection is always the same, and it is always sincere: "I have eleven employees. Every one of them does physical work. There is no light duty here." Small employers are not wrong that the problem is harder for them — they have fewer roles, no bench, no HR department, and no ability to absorb a person who cannot lift. But the consequences of not solving it are proportionally larger, because a single lost-time claim moves a small employer's experience modification factor far more than it moves a large one's.
Where Small Employers Actually Find Transitional Work
- Cross-Department Placement: The injured field technician spends six weeks in the office doing scheduling, dispatch, customer callbacks, and the estimating backlog. The work is real; it is simply not their normal work.
- The Deferred Projects List: Every small business has one. Inventory reconciliation. Digitizing paper records. Rewriting the safety manual. Photographing product for the website. Calling lapsed customers. These are genuinely valuable tasks that only get done when someone has capacity — and an injured employee on restrictions has capacity.
- Remote or Hybrid Modified Duty: If the restriction is mobility-related rather than cognitive, a phone and a laptop at the kitchen table may be a perfectly valid assignment. This option barely existed a decade ago and is now available to nearly every employer.
- Off-Site and Nonprofit Placement: A number of states and carriers permit — and some actively encourage — placing an injured worker in a temporary volunteer assignment at a local nonprofit, with the employer continuing to pay wages. The worker stays in a work routine, the wage-replacement clock stops or slows, and the community benefits. Check with your carrier and state before using this option, as the rules vary.
- Training and Certification: Restricted employees can complete safety training, forklift or equipment certification, compliance courses, or cross-training that the business has been putting off for years.
The Small Employer's Realistic Minimum
A small business does not need an enterprise program. It needs four things: a one-page written return-to-work policy, physical demand descriptions for its handful of job types, a short list of transitional tasks written down before anyone gets hurt, and a template offer letter. That is a weekend of work, and it is the difference between a $9,000 medical-only claim and a $60,000 lost-time claim that follows you through three renewals. For employers without internal HR capacity, this is precisely the kind of infrastructure a professional employer organization is built to supply — the claims coordination, the physician communication, the documentation, and the experience of having done it several thousand times before.

Statistics & Outlook
The scale of the problem is measurable, and so is the opportunity. Private industry employers reported 2.5 million nonfatal workplace injuries and illnesses in 2024 — the lowest figure in a data series going back to 2003, and a 3.1 percent decline from 2023 — at a total recordable case rate of 2.3 cases per 100 full-time equivalent workers (U.S. Bureau of Labor Statistics). Injuries are becoming less frequent. What has not improved at the same pace is what happens after one occurs.
Over the 2023–2024 period, cases involving days away from work resulted in a median of 8 days away, while the 1.1 million cases involving only days of job transfer or restriction — the return-to-work outcome — carried a median of 15 days of restricted duty and accounted for 38.5 percent of all DART cases (U.S. Bureau of Labor Statistics). Read those two numbers together and the operating logic of a return-to-work program becomes visible: the restricted-duty case is on the books longer, but the employee is at work for those 15 days rather than at home for 8-plus days and counting. The employer receives labor; the employee receives a full paycheck instead of a partial indemnity benefit; and the claim never enters the long-duration territory where costs compound.
The cost trend reinforces the urgency. NCCI reported that lost-time claim frequency declined 5 percent in accident year 2024, but that both medical and indemnity claim severity rose approximately 6 percent — meaning fewer claims, each one more expensive. (ncci.com) In an environment where severity is climbing faster than frequency is falling, duration management is the lever employers still control. The outlook for return-to-work programs is therefore one of increasing rather than decreasing importance — reinforced by an aging workforce, by the normalization of remote work as a legitimate accommodation, and by the growing recognition that prolonged absence is itself a clinical risk factor for poor recovery.
Verified Sources
- U.S. Bureau of Labor Statistics – Employer-Reported Workplace Injuries and Illnesses (2024) — Private industry employers reported 2.5 million nonfatal injuries and illnesses in 2024, down 3.1% from 2023 and the lowest in the series since 2003; total recordable case rate of 2.3 per 100 FTE workers; over 2023–2024, DAFW cases carried a median of 8 days away from work while DJTR (restriction/transfer) cases carried a median of 15 days and represented 38.5% of all DART cases. (bls.gov)
- National Safety Council / NCCI – Workers' Compensation Costs — The average cost for all workers' compensation claims combined for accidents occurring in 2022–2023 was $47,316; the most costly lost-time claims by cause were motor-vehicle crashes ($91,433), burns ($64,973), and falls or slips ($54,499). (injuryfacts.nsc.org)
- NCCI – 2025 in Sight, 2024 in Review — Accident year 2024 lost-time claim frequency declined approximately 5–6% from 2023, while indemnity claim severity rose approximately 5% and medical lost-time claim severity rose approximately 6%. (ncci.com)
- Job Accommodation Network – Costs and Benefits of Accommodations — Among employers who provided cost information on accommodations they implemented, approximately 61% reported the accommodation cost nothing, and roughly a third reported only a one-time cost; the most frequently cited benefit was retention of a valued employee. (askjan.org)
- U.S. Equal Employment Opportunity Commission – Enforcement Guidance: Workers' Compensation and the ADA — An occupational injury is not automatically an ADA disability; employers are not required to create light duty positions, but employers who reserve vacant light duty positions for occupationally injured workers must consider reassigning employees with non-occupational disabilities into them absent undue hardship. (eeoc.gov)
TrendHR - Workers' Compensation Support - TV Commercial

Technology & Tools for Return to Work
Core Platforms & Systems
The operational backbone of a modern return-to-work program is the claims management system provided by the carrier, third-party administrator, or PEO — the system of record for the claim, the reserve, the medical authorizations, and the indemnity payments. Alongside it, an HRIS tracks the employee's leave designation, FMLA entitlement, accommodation record, and transitional assignment history. The connective tissue between them is the piece most employers are missing: a restriction tracking log that records, for every open claim, the current restrictions, the assignment in place, the next medical appointment, and the review date. In small organizations, this is legitimately a well-maintained spreadsheet. In larger ones, it belongs in the HRIS or an integrated absence management platform.
Medical Communication & Job Demand Analysis
Job demand analysis tools convert job descriptions into structured physical-demand profiles — lifting thresholds, positional tolerances, frequency ratings — in a format that a treating physician can act on in the thirty seconds they will spend reading it. Some occupational clinics accept these directly into their intake workflow. Telehealth and occupational telemedicine have become a meaningful accelerator, particularly for initial triage of minor injuries and for follow-up appointments that would otherwise cost the employee half a shift in a waiting room.
Ergonomics, Prevention & Wearables
Ergonomic assessment tools — increasingly camera- or sensor-based — identify the movement patterns that produce the soft-tissue injuries that dominate workers' compensation claims. Wearable devices that flag high-risk lifting posture are moving from pilot programs into mainstream industrial use. These belong in a return-to-work discussion for two reasons: they prevent the next injury, and they help confirm that a returning employee's transitional assignment is not quietly re-creating the conditions that caused the first one.
Documentation & Forms
Templated documents are where technology earns its keep on a daily basis. A digital library containing the transitional duty offer letter, the work status report request, the physical demands job description, the FMLA designation notice, and the interactive process documentation form — with version control and electronic acknowledgment — turns an inconsistent, memory-dependent process into a repeatable one. Consistency is not just an efficiency benefit; consistency is the legal defense.
Analytics & Emerging Tools
Predictive analytics applied to claims data can flag the claims most likely to become long-duration — often keying on reporting lag, injury type, age, prior claim history, and attorney involvement — early enough for intervention to matter. This is the highest-leverage emerging application in the space, because the entire discipline of return to work rests on doing things early rather than well.

Key Performance Indicators (KPIs)
Return to work is among the most measurable functions in human resources, and the measurement is not academic — every metric below translates directly into dollars on a renewal. Organizations that track these numbers monthly can tell you whether their program works.
Core Operational KPIs
| KPI | Formula | Target |
|---|---|---|
| Return-to-Work Rate | (Injured employees returned to any duty ÷ total injured employees with restrictions) × 100 | Above 90%; below 75% indicates a structural program failure |
| Modified/Transitional Duty Utilization Rate | (Claims with a transitional assignment ÷ claims with restrictions) × 100 | Above 85%; a low rate usually means an empty job bank |
| Average Lost Days per Claim | Total days away from work ÷ number of lost-time claims | Declining trend year over year; benchmark against your industry |
| Time to First Contact | Hours between injury report and first supervisor/HR contact with the employee | Under 24 hours, without exception |
| Claim Reporting Lag | Average days between date of injury and date reported to the carrier | Under 24 hours; every day of lag raises ultimate claim cost |
| Return-to-Full-Duty Rate | (Employees released to unrestricted duty ÷ employees placed on transitional duty) × 100 | Above 90%; a low rate means transitional duty is becoming permanent |
Financial & Cost-Efficiency KPIs
| KPI | Formula | Target |
|---|---|---|
| Indemnity Cost per Claim | Total indemnity paid ÷ number of lost-time claims | Declining trend; this is the metric RTW most directly controls |
| Lost-Time Claim Ratio | (Lost-time claims ÷ total claims) × 100 | Declining trend; converting lost-time to medical-only is the core objective |
| TTD Days Paid | Total temporary total disability days paid across all open claims | Monitor monthly; every TTD day is a day RTW did not happen |
| Experience Modification Factor | Provided annually by the rating bureau (NCCI or state bureau) | Below 1.00 and trending down; a 0.85 e-mod cuts manual premium 15% |
| Average Total Cost per Claim | (Total incurred medical + indemnity) ÷ number of claims | Track against industry benchmark; watch the trend, not the single year |
Quality, Safety & Emerging KPIs
| KPI | Description | Target |
|---|---|---|
| DART Rate | (Number of DART cases × 200,000) ÷ total hours worked — the OSHA measure of cases involving days away, restriction, or transfer | At or below your industry's published rate |
| Re-Injury / Recurrence Rate | Percentage of returning employees who suffer a recurrence of the same injury | Under 5%; a high rate means assignments are exceeding restrictions |
| Retention After Injury | Percentage of injured employees still employed 12 months after their injury date | Comparable to your general retention rate; a large gap is a warning sign |
| Litigation Rate | Percentage of claims involving attorney representation | Below industry average; correlates strongly with slow first contact |
| Claim Closure Rate | Percentage of claims closed within 12 months of the injury date | High and improving; open claims accrue reserve and rating impact |
Review operational KPIs monthly and financial KPIs quarterly. Review your experience modification worksheet the moment it arrives — not at renewal — because that document tells you exactly which claims are costing you premium and gives you the window to correct reserves that no longer reflect reality.

Why Return-to-Work Programs Fail
Most failed programs are not missing a policy. They have one. What they are missing is execution at the five points below — and every one of these failures is entirely within the employer's control.
- Make-Work Assignments. Counting bolts. Sweeping a floor that was swept an hour ago. Sitting in a break room "in case someone needs something." Employees know when they are being warehoused, and so do their coworkers. Make-work signals that the company does not actually value the employee's contribution, which is precisely the message that pushes an injured worker toward an attorney. If the task would not be worth paying for on an ordinary day, do not assign it.
- Verbal-Only Offers. An offer of transitional work that exists only in the memory of a supervisor is unenforceable, undocumentable, and invisible to the adjuster who needs it to adjust benefits. It also cannot be defended if the employee later claims no offer was made. Write it down, date it, and distribute it.
- No End Date. Transitional duty without an expiration date becomes a permanent position by accretion. Six months later the employee has been doing modified work for so long that removing it looks like an adverse action, and the employer has inadvertently created exactly the permanent light duty role it never wanted to staff.
- Supervisor Resistance. The program lives or dies on the floor. A supervisor who treats the returning employee as dead weight, who complains about carrying them, or who quietly pressures them to exceed restrictions will destroy in one shift what HR built in six months. Supervisors need to be trained, held accountable, and — critically — not penalized in their own productivity metrics for hosting a transitional assignment.
- Silence During the Absence. Prolonged silence tells an injured worker they have been written off. The correlation between early, warm, consistent contact and claim outcomes is one of the most consistent findings in the field — and it costs nothing.

When the Employee Can't Return
Not every claim ends with a full-duty release. These are the scenarios employers fear most, and they are where a documented process matters more than anywhere else — because these are the fact patterns that become lawsuits.
Permanent Restrictions at MMI
When the treating physician determines the employee has reached maximum medical improvement with permanent restrictions, the workers' compensation question (what is the disability rating and what benefits are owed?) and the employment question (can this person still do this job?) separate. The ADA analysis now takes over. Can the employee perform the essential functions of their position with a reasonable accommodation? If not, is there a vacant position for which they are qualified? Reassignment is a form of reasonable accommodation, and the employer must consider it before concluding that separation is the only option. What the employer may not do is skip this analysis because a comp rating says "permanently partially disabled."
The Employee Refuses the Transitional Assignment
An employee cannot be compelled to accept light duty in lieu of FMLA leave. But in most states, refusing a valid, suitable offer of transitional work — one that is within the physician's restrictions, at a reasonable location, and appropriately compensated — will suspend or reduce their workers' compensation indemnity benefits. This is why the written offer matters so much: the offer letter is the document that establishes the offer was valid and suitable. Coordinate with the adjuster before taking any action, and never treat a refusal as automatic grounds for termination without legal review.
The Employee Exhausts FMLA and Still Cannot Work
Exhausting the 12-week FMLA entitlement does not end the analysis. Additional leave may itself be a reasonable accommodation under the ADA if it is finite, definite, and does not impose an undue hardship. An automatic termination policy triggered by FMLA exhaustion is one of the most frequently litigated employer practices in this area. Indefinite leave, however, is generally not a required accommodation — the distinction is whether the employee can articulate a reasonably certain return date.
Separation
Separation is sometimes the correct and lawful outcome. It becomes a liability when it is undocumented, when it skips the interactive process, when it follows suspiciously fast on the heels of a claim filing, or when the employer applied a rigid rule — a "100% healed" policy, an automatic termination at 90 days — instead of an individualized assessment. Before separating an employee with an open workers' compensation claim, document the accommodation analysis, confirm no vacant position exists, and have the decision reviewed by counsel.

Frequently Asked Questions
How soon can an injured employee return to work?
An injured employee can return to work as soon as the treating physician issues restrictions the employer is able to accommodate — which is frequently far earlier than employers assume, and often without any lost days at all. The controlling document is the work status report, not the severity of the injury as it appears to the employer.
The practical constraint is rarely medical; it is informational. Physicians write "off work" as a default when they do not know what the job involves and have no assurance that the employer can accommodate anything less than full duty. Sending the treating physician a written physical-demands job description together with a copy of the company's transitional duty policy changes the calculus at the first appointment. Speed matters because duration is self-reinforcing: the longer an employee is out of the workplace, the more likely secondary complications and attorney involvement become, and the lower the probability of a return at all. The employer's window of maximum influence is the first 24 to 72 hours.
Can I require an employee to accept light duty?
You cannot compel an employee to report to a light duty assignment, and you cannot require them to accept light duty in place of FMLA leave if they are FMLA-eligible. What you can do is make a valid, written offer of suitable transitional work — and in most states, an employee who refuses such an offer will have their workers' compensation indemnity benefits suspended or reduced as a result.
The distinction is between the employee's leave rights and their wage-replacement benefits. Under the FMLA, light duty work does not count against the 12-week entitlement, and an employee retains the right to decline it and remain on protected leave. Under state workers' compensation law, however, indemnity benefits exist to replace wages the employee cannot earn — and if suitable work within their restrictions has been offered and declined, the rationale for those payments largely disappears. For the offer to have this effect, it generally must be in writing, within the documented restrictions, at a reasonable location, and appropriately compensated. State rules vary meaningfully, so coordinate with your claims adjuster before acting on a refusal.
What if the doctor won't release the employee to return?
If a physician will not release an employee to any form of work, the first question to ask is whether the physician has actually seen what the work involves. In a large share of cases the answer is no — and the "no release" is a conservative default rather than a considered judgment about a specific set of tasks.
The first move is always to provide better information: a written physical-demands description of the proposed transitional assignment, listing exactly what the employee would and would not be asked to do, along with confirmation that the employer will enforce the restrictions. A nurse case manager, where one is assigned, can often obtain clarification quickly. If a genuine dispute remains, a functional capacity evaluation, an independent medical examination, or a second opinion within the carrier's network may be options depending on your state. What the employer must not do is pressure the employee to work outside their restrictions or attempt to go around the physician.
Does light duty have to be a real job?
Yes — and this is the point at which most return-to-work programs quietly break. Transitional duty must consist of productive work that the business genuinely needs performed. Manufactured busywork is bad for the claim, bad for the employee, and bad for the culture of the workplace.
There are two reasons this matters. The first is human: employees know when they are being warehoused, and that message is one of the most reliable predictors of attorney involvement in a claim. The second is legal: a make-work assignment is harder to defend as a valid, suitable offer of employment if the assignment is ever challenged. The solution is preparation, not improvisation. Build a transitional duty job bank in advance — inventory counts, safety audits, equipment inspection logs, document digitization, customer follow-up calls, training and certification, deferred projects. These are real tasks with real value, and an employee performing them is making a genuine contribution while they heal.
Can I terminate someone on workers' compensation?
An open workers' compensation claim is not a shield against every employment action — but terminating an employee with an active claim is one of the highest-risk decisions an employer can make, and it should never be done without documentation and legal review.
Nearly every state prohibits retaliation against an employee for filing a claim, and courts examine the timeline closely: a termination that closely follows a claim filing invites the inference of retaliation regardless of the stated reason. Layered on top are the ADA and, where applicable, the FMLA. Before any separation, an employer should be able to demonstrate that it engaged in the interactive process, considered reasonable accommodations including reassignment to a vacant position, did not apply a rigid rule such as a "100% healed" requirement, and that the reason for separation is documented, legitimate, and consistently applied to employees without claims.
Do restricted-duty days count on the OSHA 300 log?
Yes. Returning an injured employee to restricted or transitional duty does not remove the case from your OSHA 300 log. The case remains recordable and is recorded as a job transfer or restriction case, with the days of restriction counted — capped at 180 calendar days.
This surprises employers who believe a return-to-work program will improve their recordable injury statistics. It will not, and using transitional duty to keep cases off the log — or pressuring a physician to avoid issuing restrictions — is a recordkeeping violation. What return to work actually improves is the days-away-from-work count, the claim cost, the claim duration, and the experience modification factor. Those are the real financial levers. Both a lost-time case and a restricted-duty case appear in your DART count; only one of them costs you a premium increase for three years.
Key Takeaways
A return-to-work program is the single highest-leverage workers' compensation control an employer has, because it is the only one that operates on claim duration — and duration is what turns an ordinary injury into an expensive one. The mechanics are unglamorous and entirely repeatable: report the injury within 24 hours, contact the employee immediately, send the physician a physical-demands job description, obtain the work status report, match the restrictions to a pre-built transitional assignment, and put the offer in writing with a defined end date.
The legal complexity is real but manageable. A single work injury can simultaneously trigger state workers' compensation law, the ADA, and the FMLA, and compliance with one does not satisfy the others. Designate FMLA in writing, run and document the ADA interactive process when restrictions are significant or permanent, retire any "100% healed" policy, and record restricted-duty days honestly on the OSHA 300 log.
Programs fail on the human details, not the legal ones — make-work assignments, verbal offers, open-ended duty with no end date, an unsupportive supervisor, and silence during the absence. Employers who get those five things right convert lost-time claims into medical-only claims, protect their experience modification factor for years, and keep experienced people on the payroll instead of losing them to an injury that never had to end a career.










")
")









")

